 Search Articles
Search Articles


WASHINGTON (CN) — Doctors take an oath to preserve life to the best of their ability. Neither skill nor desperation can manifest a ventilator, however, in the coming days when facilities across the country exhaust their supplies to treat the surging population of Americans becoming sick with Covid-19.
The respiratory disease caused by novel coronavirus has infected over a million people globally and killed more 73,000 since first emerging in China last December. At its most fatal, without the assistance of a lifesaving ventilator, the virus grips its victims with an agonizing asphyxia. Survivors of acute infections liken the experience to having ground glass in the lungs.
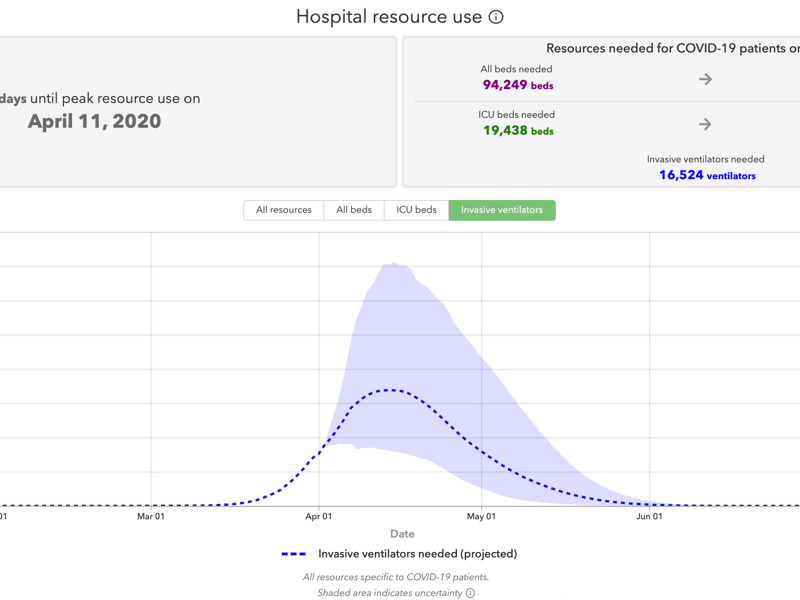
The United States will reach peak use of its ventilator supply on Saturday, April 11, according to a forecast continuously updated by the Institute for Health Metrics and Evaluation, part of University of Washington Medicine.
And with each new wave of patients seeking care, American doctors and nurses are brought closer to a harrowing dilemma they likely heard about last month from their brethren in Italy — whose early experience with the virus offered for many nations a case study in pandemic response — about whose life will be supported with a ventilator or who will wait, and potentially die, as a result.
To meet demand, President Donald Trump tasked companies like General Motors and Ford with manufacturing 100,000 ventilators in 100 days. Neither company got started, however, before this week. Ford expects to have produced just 1,500 ventilators by April’s end. By mid-May, GM says it could produce 10,000 ventilators per month.
As for the strategic national stockpile, the Federal Emergency Management Agency shared documents with Congress last week indicating that just 9,500 ventilators were left. Those stocks are now totally depleted, the Health and Human Services Department confirmed Monday to the House Oversight Committee, as demand continues to rise.
The circumstances are far from ideal, and it may very well be that the first leg of a rationing race in one of the world’s wealthiest nations has already been lost. On this, only time will tell. Physicians in the meantime will rely on their own prowess and their state’s rationing guidance where and if it exists. Most states offer protocols, but there are no federal recommendations to anchor them.
Neither the White House nor the Health and Human and Services Department returned multiple requests for comment.

“The impulse of physicians is always, and ought to always be, to care for the sick and vulnerable,” said Dr. Daniel Sulmasy, professor of biomedical ethics at Georgetown University where he is also acting director of the Kennedy Institute of Ethics. “We hope we can avoid rationing, but if not, a fair way of doing it must be based on a combination of need, prognosis and the chance of actually benefiting or surviving.”
Those issues are typically applied against a scoring system with criteria varying from state to state. The criteria for and against access to ventilators consider diverse factors including pregnancy, Alzheimer’s disease or even status as a first responder to the pandemic.
Under the best circumstances in medicine, the utilitarian approach — achieving the greatest good for the greatest number of people — poses its own difficulties. In crisis, the premise becomes even complicated.
As hospital systems feel the full weight of coronavirus response, for example, the Health and Human Services Department Office for Civil Rights issued a stark warning to doctors on disability discrimination when confronting expected supply shortages.
Care cannot be denied to a person with a disability on the basis of “stereotypes, assessments of quality of life, or judgments about a person’s relative worth based on the presence or absence of disabilities,” the guidance states.
The call for protections does not perfectly align, however, with many existing recommendations for doctors in states like in Alabama where they are directed, in some instances, to categorize patients with issues like severe mental retardation, dementia or severe traumatic brain injury as low-ranked candidates for ventilator support.
These types of recommendations are informed by members of the scientific, medical and public health communities — sometimes with public input, though that is less frequent and typically only prompted after major events like a natural disaster or a bioterrorist attack.
Back in 2007, when she was a visiting professor at Johns Hopkins University, Shelley Hearne published recommendations, now eerily prescient, on the need for regular infectious disease reporting.
“In times of heightened medical threats, if the nation’s health agencies are to exhibit national leadership, they must have more rapid response mechanisms,” wrote Hearne, who is now the Alfred Sommer and Michael Klag Decanal professor of the practice for public health advocacy and director of the school’s Center for Public Health Advocacy.
“They can still draw on the advice and counsel of key scientists and constituency groups,” Hearne wrote, “but the authority for quick, directive action on nationwide disease reporting should exist on the national level.”
Reflecting on those years advising the federal government, Hearne spoke about the frustration of having her suggestions fall on deaf ears.
“There were lessons learned and plans prepared,” she said last week in an interview. “We’re not following that playbook now and we are in bad straits. Really, a lot of this could have been prevented. It’s a bit horrifying.”
Discussions of rationing often bring up criticism of doctors “playing God,” making it a subject matter that requires considerable trust from the outset between the public and doctors, doctors and health systems, and health systems and states.
“There is absolutely nothing worse than the loss of the public trust in government decision making in an emergency. It’s just what we’re facing now,” Hearne said.
One way the inherent dangers that come with an overreliance on improvisation is reflected, she added, is how various federal agencies offered conflicting messaging since the start of the outbreak on the virus, testing, and the accessibility of personal protective equipment and ventilators.
“Public health has had equal-opportunity neglect from Democrats, Republicans, independents,” she said. “It’s been a Cinderella for a long time. … I’m assuming when we get through this — and we’re talking a long way away, many months, it may even be a few years — but this will be the wakeup call of a lifetime for a generation. I think there will be a number of reforms. But I’ve come to learn, I can’t always guess how they might manifest themselves.”
While politicking unfolds, doctors await the next crush of patients and hope regional infection curves flatten so they and their resources are not completely overwhelmed.
The New England Journal of Medicine reported in March some hospitals may consider forming “rapid response bioethics teams” to assist physicians in the event of a ventilator shortage. This could potentially allow doctors to spend precious minutes on treatment instead of becoming bogged down in hundreds of pages of rationing guidance in a tough scenario where, for example, a doctor might be forced to decide whether to keep a 20-year-old with advanced kidney disease and cancer on a ventilator or someone who may be 70 but fit.
Sulmasy, the Georgetown bioethicist, said this sort of delegating would be “quite reasonable” in the event of an acute shortage.
“It would be done in order to make sure the people who are caring for the patient can focus on that and not have to worry about the guilt of having decided if this person is not going to be on a ventilator and another person will,” Sulmasy said in an interview.

It already exists in some form, he said, giving the example of clinicians who consult family members of patients with severe brain damage and a low survival rate. In a pandemic, a rapid response ethics team could be a salve for weary doctors.
Ideally, these “ethical triage units” would be arranged in advance of a pandemic. For now, however, the emphasis for hospitals that create these teams should be on ensuring that rationing decisions are not left to one triage officer.
Rather, there should be a panel with combined expertise in ethics and critical care. Shifting these people around will also be necessary. After all, Sulmasy pondered, who triages the triage unit?
“There could be criticism they’re playing God, or people who aren’t caring for the patient shouldn’t be the ones making the decision, or that they can’t fine-tune it enough,” he said. “Those are possible arguments, but in the interest of fairness and preserving the best care for patients who do get on the ventilators, this could be the best kind of way of doing that.”
Even marginally shielding doctors from this strain could be hugely helpful because care providers are not just in physically demanding situations but ethically and emotionally dicey ones, too.
“It’s difficult to wear masks or don gowns when seeing patients all the time,” he said. “You lose eye contact through shields, and the ability to touch a patient with gloves. All of that is sort of strange in most cases, and dealing with potential shortages adds to that.”
The oath a doctor takes states, Sulmasy recalled, “I will apply dietetic measures for the benefit of patients to the best of my ability, keeping them from harm.”
The ethical dilemma doctor may soon face rests on that four words: “the best of my ability.”
“When there is an acute shortage, one’s ability is limited, so one does the best one can,” Sulmasy said. “The philosopher Immanuel Kant argued that ‘ought implies can.’ One can only have a moral duty to do what is possible. If there is only ventilator and two people need it, one cannot treat both.”
Subscribe to our free newsletters
Our weekly newsletter Closing Arguments offers the latest about ongoing trials, major litigation and rulings in courthouses around the U.S. and the world, while the monthly Under the Lights dishes the legal dirt from Hollywood, sports, Big Tech and the arts.